Do you have a fear of vomiting? Does your fear of vomiting impact your ability to eat certain foods, in certain situations, or to an adequate level of fullness? If you have been diagnosed with a restrictive eating disorder, this phobia may drive your eating.
You have probably heard of arachnophobia (fear of spiders), agoraphobia (fear of open spaces), claustrophobia (fear of enclosed spaces), or glossophobia (fear of public speaking), but have you heard of emetophobia? Emetophobia is the specific fear of vomiting (SPOV). It is a diagnosable disorder categorized in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, text-revision (DSM-5-TR) as specific phobia, “other” subtype.
Emetophobia refers to an intense and irrational (or out of proportion) fear of vomiting. It also encompasses avoidance of situations that could lead to vomiting or interacting with vomit. This specific fear of vomiting goes above and beyond a disgust for vomiting.
People with emetophobia will often avoid food, sensations (i.e., feelings of fullness, spinning motion, etc.), and situations that they associate with vomit. Avoidance of feelings of fullness or foods related to vomiting can lead to inadequate nutritional intake. Undereating, in turn, can lead to medical consequences associated with malnutrition, significant weight loss, and/or significant impairment to occupational or social functioning. Professionals may not accurately diagnose emetophobia, mistaking it for a restrictive eating disorder, such as anorexia nervosa.
While emetophobia and eating disorders–especially Avoidant/Restrictive Food Intake Disorder (ARFID) fear type– can occur together, it is essential to receive the appropriate treatment for emetophobia as well.
Research on emetophobia is limited. Of what we know, emetophobia most commonly develops in childhood or adolescence and appears to impact females more than males. However, an acute onset is possible after an aversive experience, such as food poisoning or a medical issue. Emetophobia is challenging to treat due to a high drop-out rate or poor treatment response. Emetophobia may be the most common specific phobia for which people seek treatment. Left untreated, it can become one of the most impairing phobias because people with it come to avoid such a broad range of situations.
Symptoms of emetophobia include behaviors, thoughts, experiences of anxiety, physical symptoms, and impact on daily living.
Avoidance may include avoidance of sensations and situations.
People with emetophobia may avoid places and situations where they believe vomiting is more likely to occur. Situations and places may include people drinking alcohol, like bars or sporting events, medical facilities, or people who have recently been sick or around people who are ill. People with emetophobia may also isolate socially due to the fear of others being sick.
People with emetophobia may engage in many safety behaviors to try to prevent vomiting. Some of these behaviors include:
People with emetophobia often experience impairment in their social, occupational, or medical functioning due to several factors. The fear of vomiting and the safety behaviors that people with emetophobia engage in can cause someone to become socially isolated. They may avoid social situations or even work-related duties. Alternatively, they may frequently call out sick. In addition to the social and occupational impairment, someone who is avoiding eating may suffer from the medical consequences of malnutrition.
People with emetophobia feel terrified thinking about vomit or vomiting and experience intrusive and obsessive thoughts about vomiting. The thoughts may be related to fear of others vomiting, or the person with emetophobia vomiting, or vomit in general.
The two most commonly used validated measures to assess emetophobia are the Specific Phobia of Vomiting Inventory (SPOVI) and the Emetophobia Questionnaire (EMET Q-13).
Emetophobia and an eating disorder like anorexia nervosa, bulimia nervosa, or ARFID can co-occur. One study found that one-third of people in the survey with emetophobia also engaged in restriction and abnormal eating behaviors. In another study, 80% of individuals with emetophobia endorsed disordered eating behaviors. Another study found that 131 participants were diagnosed with comorbid anorexia nervosa.
People with emetophobia commonly restrict the volume or type of food they eat to reduce the chances of vomiting or becoming sick. This fear-based restriction of food intake may overlap with ARFID. According to the DSM-5-TR, ARFID is an eating disorder in which individuals fail to meet their nutritional needs but lack the typical body image concerns and fear of weight gain that individuals with anorexia nervosa endorse. People with emetophobia may also meet criteria for ARFID when there is a significant fear of vomiting and eating is restricted, and any one of the following conditions is met:
Over time, individuals with emetophobia who engage in restriction of food intake may meet criteria for ARFID due to the impact on their medical or psychosocial functioning. Individuals with emetophobia may also develop symptoms of anorexia nervosa, such as concerns with their weight and shape, negative body image/ fear of weight gain, or the avoidance of more calorically dense foods.
To ensure correct diagnosis, clinicians should attempt to understand the rationale for the avoidance of food and assess appropriately for concerns with body image and other factors that may contribute to the avoidance of food.
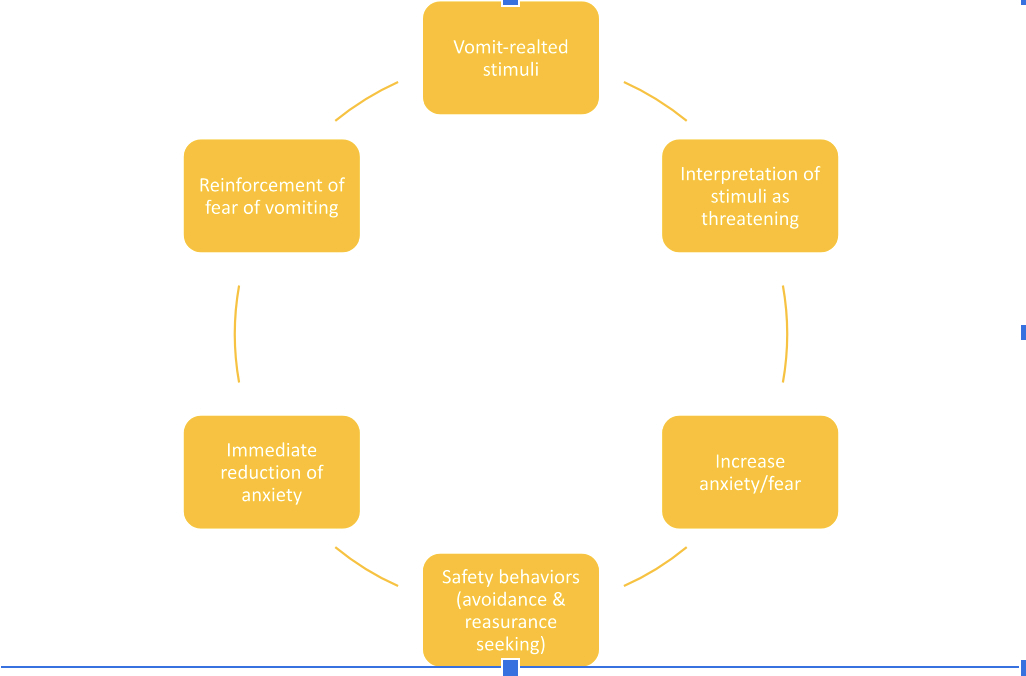
Anxiety and avoidance behaviors (including safety behaviors) as well as hyperawareness, maintain emetophobia.
In the emetophobia cycle depicted below, the person encounters something related to vomiting. Through a conditioned response, they interpret this as something dangerous or scary, which then increases their fear. The person then engages in safety behaviors such as avoidance or reassurance seeking, which in turn reinforces the fear of vomiting. Safety behaviors provide a false sense of control over vomiting and only offer temporary relief.
An example could be: A person sees their friend who looks unwell and says that they are feeling nauseous. The person interprets the situation as the friend is sick and will vomit. Or they might believe the friend is ill and they are going to catch their illness and vomit. The person becomes anxious and leaves the situation, avoiding other social interactions with this friend.
Common avoidance behaviors include
Examples of reassurance-seeking behaviors include:
Other examples of safety behaviors include:
Heightened attention to bodily sensations also maintains emetophobia. People with emetophobia may pay more attention to their body, especially gastrointestinal symptoms, and are more likely to interpret these symptoms as nausea. Anxiety can create symptoms of gastrointestinal distress, as described above, and can be misinterpreted as a precursor for vomiting, which can increase anxiety in someone with emetophobia.
Exposure and Response Prevention (ERP) is an evidence-based treatment approach for emetophobia.
Before beginning treatment, psychoeducation about emetophobia is provided, including information about phobias, the emetophobia cycle, the cycle of anxiety, safety behaviors, and other important information.
The pre-treatment phase will also include assessment of symptoms using a measure such as the SPOVI or the EmetQ-13.
ERP involves creating a fear hierarchy – this involves listing situations, food, places, physical feelings, etc., in order of least anxiety-provoking to most anxiety-provoking – this can include saying vomit words, watching videos of others vomiting, creating the physical feeling of vomiting, etc. Often, you will list these on a scale from one to ten.
Individuals are then gradually exposed to these situations in one of three ways. 1) in vivo exposures – exposures that take place in real time, 2) imaginal exposures – imagining the situation, and 3) interoceptive exposure – exposure to the physiological sensations. Unlike many other phobias, exposures do not include forcing the individual to face the exact situation they are afraid of (vomiting). Instead, exposures focus on the sensation of vomiting through interoceptive exposures and situations that may include being around places where others are more likely to be sick or vomit, or watching videos of vomiting.
People are prevented from engaging in safety behaviors, such as escaping, checking expiration dates, and excessive sanitizing. People rate their subjective units of distress (SUDS) to communicate their level of distress during these exposures. ERP is beneficial in the treatment of emetophobia as it helps to reduce avoidance and safety behaviors that cause decreased ability to function. ERP enables the creation of new associations with previously feared situations. By contrast, when people avoid, they fail to recognize new information and disconfirm their fears or learn that they can handle the situation.
Suppose a person with emetophobia is at a low weight. In that case, weight gain and restoration of regular patterns of eating are essential treatment goals, just as it is in anorexia nervosa. Family-based treatment focused on anxiety and feeding management may be a good treatment choice for teens needing to restore weight.
Carly Poynter, Psy.D., Lauren Muhlheim, Psy.D., and several other of our therapists have specialized training and experience in treating emetophobia. Complete the EDTLA contact form to get connected with one of our emetophobia specialist therapists and begin your recovery.
If someone you care about struggles with emetophobia, it can be difficult to fully grasp how intense their fear is. You might see their reactions as unreasonable and feel the urge to lighten the mood with jokes or encourage them to move past it. While they often recognize that their fear doesn’t make logical sense, simply knowing that isn’t enough to make it go away. They’re also aware that their phobia can be frustrating for you, and they often feel ashamed when it affects not just them—but those around them, too. Learn how you can support your loved one with emetophobia.
Höller, Yvonne, Mark van Overveld, Heili Jutglar, and Eugen Trinka. 2013. “Nausea in Specific Phobia of Vomiting.” Behavioral Sciences 3 (3): 445–58.
Hout, Wiljo J. P. J. van, and Theo K. Bouman. 2012. “Clinical Features, Prevalence and Psychiatric Complaints in Subjects with Fear of Vomiting.” Clinical Psychology & Psychotherapy 19 (6): 531–39.
Hunter, Paulette V., and Martin Antony. 2009. “Cognitive–behavioral treatment of emetophobia: The role of interoceptive exposure.” Cognitive and Behavioral Practice, 16: 84–91.
Keys, Alexandra, and David Veale. 2018. Atypical Eating Disorders and Specific Phobia of Vomiting. Clinical Handbook of Complex and Atypical Eating Disorders. 189-204. Oxford University Press. New York.
Keyes, A., Gilpin, H. R., & Veale, D. (2018). Phenomenology, epidemiology, co-morbidity, and treatment of a specific phobia of vomiting: A systematic review of an understudied disorder. Clinical Psychology Review, 60, 15–31.
Maack, Danielle J., Brett J. Deacon, and Mimi Zhao. 2013. “Exposure Therapy for Emetophobia: A Case Study with Three-Year Follow-Up.” Journal of Anxiety Disorders 27 (5): 527–34.
Riddle-Walker, Lori, David Veale, Cynthia Chapman, Frank Ogle, Donna Rosko, Sadia Najmi, Lana M. Walker, Pete Maceachern, and Thomas Hicks. 2016. “Cognitive Behaviour Therapy for Specific Phobia of Vomiting (Emetophobia): A Pilot Randomized Controlled Trial.” Journal of Anxiety Disorders 43 (October): 14–22.
Veale, David. 2009. “Cognitive Behaviour Therapy for a Specific Phobia of Vomiting.” The Cognitive Behaviour Therapist 2 (4): 272–88.
Veale, David, Philip Murphy, Nell Ellison, Natalie Kanakam, and Ana Costa. 2013. “Autobiographical Memories of Vomiting in People with a Specific Phobia of Vomiting (Emetophobia).” Journal of Behavior Therapy and Experimental Psychiatry 44 (1): 14–20.
TL; DR Dieting and strict dietary rules can create emotional and physical deprivation, leading to…
TL; DR Nutritional supplement shakes play a vital role in eating disorder recovery by helping…
TL; DR Emetophobia is an intense fear of vomiting that can severely limit a person's…
TL; DR In Family-Based Treatment, parents play a crucial role in helping their teens recover…
TL; DR Transitioning to college can be especially challenging for young adults with eating disorders.…
TL;DR Online Family-Based Treatment (FBT) is a highly effective therapy for teens with eating disorders,…
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}